Systems Over Recruitment: A Strategic Framework for Clinical Retention and Quality Assurance in Senior Healthcare

Executive Summary: The False Promise of the "Recruitment Chase"
The long-term care and senior living sector is navigating a profound transformation driven by shifting regulatory frameworks, severe financial pressures, and structural labor shortages. Historically, healthcare administrators have responded to staffing shortages through an intensive focus on recruitment, relying heavily on signing bonuses, aggressive hiring campaigns, and temporary agency personnel.
However, empirical evidence suggests that this recruitment-focused approach fails to resolve the underlying systemic vulnerabilities that drive clinical turnover. Most healthcare organizations are completely addicted to chasing. More signing bonuses. More travel agencies. More job boards. Chasing.
Prioritizing the current workforce through robust operational systems, structured professional development, and supportive environments yields far greater stability and superior resident outcomes. An intensive focus on internal clinical teams demonstrates that an organization values resilient systems over the constant chase of recruitment. This is why we argue the operator-level case for autonomous hiring is crucial: it shifts the talent strategy from a chaotic manual process to an automated engine.
Healthcare leadership can establish a workplace clinicians choose to stay in by replacing reactive practices with structured, operations-driven operational models. This transition from an HR-centric recruitment focus to an operations-driven retention culture is critical in the current macroeconomic and regulatory environment.
When you build a system that supports your current clinicians, the market takes notice. That is the difference between begging for candidates and becoming the obvious choice. Build something worth finding.
The Macroeconomic and Regulatory Landscape of Senior Care
In late 2025, the Centers for Medicare & Medicaid Services (CMS) repealed proposed federal minimum staffing requirements, including the prescriptive hours per resident day thresholds and the mandate for a 24/7 on-site registered nurse. While this regulatory shift offers operators greater operational flexibility to design staffing models aligned with local labor realities, it simultaneously demands a more sophisticated approach to clinical workforce stability. The pressure hasn't left the building; the responsibility has simply shifted to your operational infrastructure.
Furthermore, the enactment of HR 1 in July 2025 is projected to cut over $900 billion from the Medicaid program over ten years, leading to state-level funding reductions of 4% to 20%. Because Medicaid remains the primary payer for more than 60% of nursing home stays, senior care facilities must optimize internal retention systems to protect their margins from the high costs of clinical attrition.
Beyond the direct financial ledger, turnover degrades clinical quality and operational continuity. Frequent staff changes disrupt the highly personal "rhythm of care" required by older adults, who depend on familiar caregivers to recognize subtle changes in their baseline physical or cognitive status. Research published in JAMA Internal Medicine established that within-facility variation in staff turnover is directly associated with decreased nursing home care quality. High attrition rates correlate with elevated rates of resident falls, pressure ulcers, urinary tract infections, rehospitalizations, and overall resident mortality.
The Real Cost Breakdown by Role
Registered Nurse (RN)
- National Median PBJ Turnover Rate: 102.9%
- Replacement Cost per Employee: $37,700 - $61,000
- Primary Quality and Clinical Vulnerabilities: Loss of clinical leadership, increased rehospitalization rates, elevated pressure ulcers, and a 7% higher permanent attrition rate when agency staff are heavily utilized.
Licensed Practical Nurse (LPN)
- National Median PBJ Turnover Rate: 79.8%
- Replacement Cost per Employee: Highly variable based on local market
- Primary Quality and Clinical Vulnerabilities: Disruption of routine clinical treatments, increased supervisory burden on remaining RNs, and elevated medication administration risk.
Certified Nursing Assistant (CNA)
- National Median PBJ Turnover Rate: 98.8%
- Replacement Cost per Employee: ~$2,600
- Primary Quality and Clinical Vulnerabilities: Inconsistent assistance with activities of daily living (ADLs), elevated resident falls, higher infection rates, and degraded resident-family trust.
Longitudinal studies reveal that nursing homes categorized as high utilizers of agency staff experience a 7% higher turnover rate among permanent RNs and a 1.9% higher turnover rate among permanent CNAs compared to low-utilizer facilities. This relationship is driven by several operational and psychological mechanisms:
- Operational Burden: Because agency nurses are unfamiliar with a facility’s specific clinical protocols, physical layout, and resident care plans, permanent RNs must absorb a higher cognitive and physical workload to guide, monitor, and support them, accelerating permanent staff burnout.
- Perceived Inequity: Permanent staff frequently compare their compensation and workload to those of contract workers, who often earn significantly higher hourly wages for identical or less integrated duties. This perceived disparity fosters demoralization and prompts permanent staff to either demand wage increases or exit the facility.
- Disruption of Team Cohesion: Effective clinical care relies on shared mental models and mutual trust. A rotating door of transient contract staff prevents the formation of cohesive clinical teams, leading to communication breakdowns and a heightened risk of medical errors.
- Quality and Rating Impact: Staffing stability is a direct driver of clinical excellence. Analysis indicates a clear relationship between temporary labor and regulatory performance: in 2024, facilities rated with a single star under the CMS Five-Star Quality Rating System relied on an average of 8.5% contract labor, whereas five-star facilities utilized only 4.4% contract labor.
These findings demonstrate that while agency labor offers a buffer against short-term absenteeism, over-reliance on contract staff creates a cycle of permanent staff attrition and increasing operational costs. To break this cycle, healthcare organizations must shift resources from temporary labor acquisition to sustainable internal retention frameworks.
Formulating a Weighted Care-Hour Turnover Metric
To accurately assess the impact of staffing on clinical quality, organizations must move away from simple annual averages and adopt the weighted, care-hour-based turnover metric utilized by CMS and academic researchers. This calculation recognizes that the departure of a full-time clinician who provides a large volume of direct care hours is significantly more disruptive to a facility than the departure of a part-time or transient employee.
By tracking this weighted metric alongside role-specific, shift-level, and unit-level trends, administrators can deploy targeted retention strategies where care continuity is most vulnerable. Stop looking at broad, high-level HR spreadsheets that mask the bleeding. If a full-time overnight RN leaves, your system takes a massive hit compared to a part-time weekend float. Measure the care hours, because that is where your operational risk lives.
For operators looking to benchmark these standards against nationwide metrics, LeadingAge provides comprehensive data and policy frameworks updating senior care metrics for the 2026 operational landscape.
Developing Multi-Tiered CNA Career Ladders and Upskilling Pathways
The lack of defined career progression is a primary driver of attrition among frontline caregivers, particularly CNAs. Research from the Moving Forward Coalition indicates that advancing certified career pathways is one of the most immediate and impactful levers for stabilizing the long-term care workforce. Developing a formal career ladder transitions the CNA role from a high-turnover, entry-level job into a professionalized career path, boosting morale, improving training quality, and enhancing retention without disrupting the facility's licensed nursing mix.
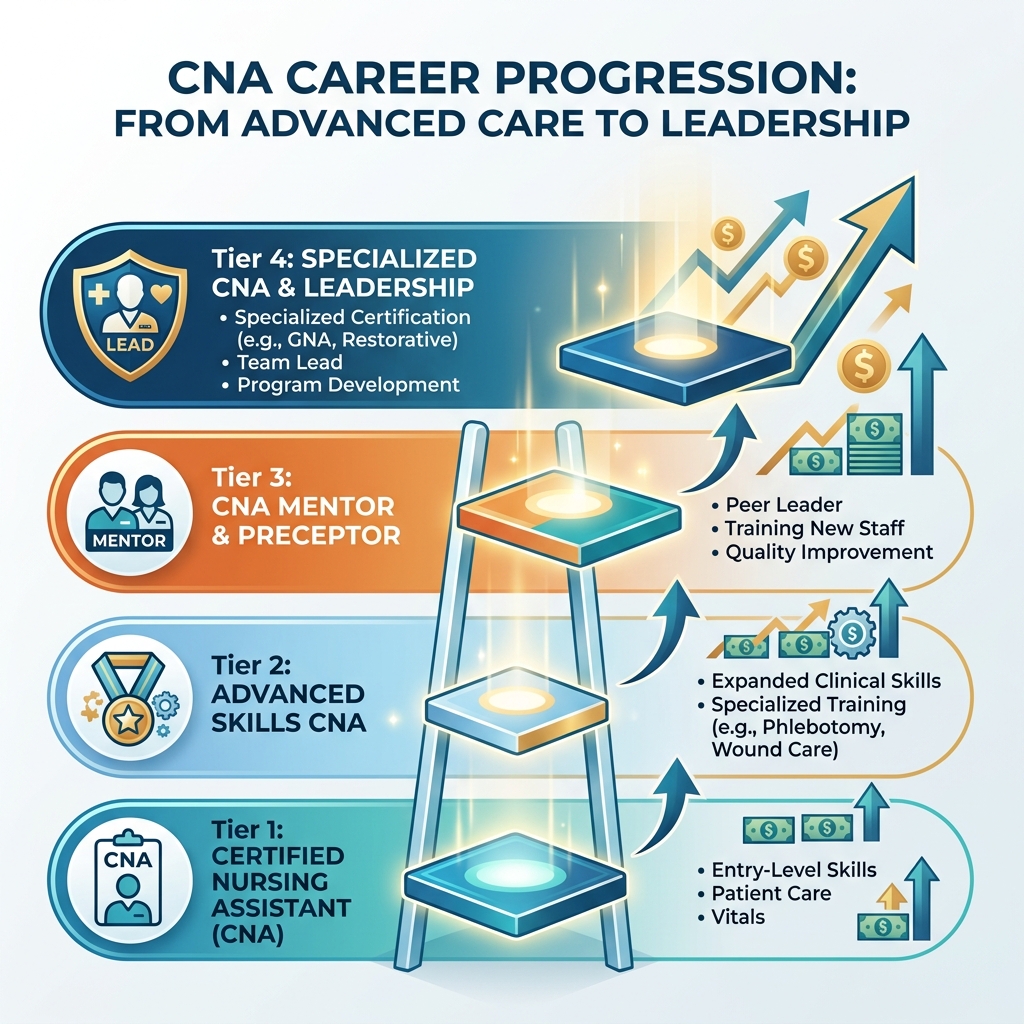
To implement a multi-tiered career ladder framework that drives retention, senior care executives should establish a structured pathway modeled after successful state initiatives:
- CNA Tier 1 (Entry Level): Core certification focusing on basic activities of daily living (ADLs), resident safety, and foundational documentation.
- CNA Tier 2 (Advanced Caregiver): Focuses on specialized competencies such as restorative nursing interventions, advanced dementia care, and localized behavioral management.
- CNA Tier 3 (Mentor / Preceptor): Cross-trained in peer leadership, clinical shadowing protocols, and new-hire performance tracking.
- CNA Tier 4 (Specialized Medication/Clinical Aide): Competency-based upskilling focused on Qualified Medication Aide delegation or advanced healthcare coordination, depending on state regulations.
Every step up the ladder must be directly tied to automatic, transparent wage adjustments and expanded clinical responsibilities. When your frontline staff can map out their next three years of financial and professional growth inside your walls, they stop browsing job boards for an extra fifty cents an hour.
Decentralized and Person-Directed Models of Care
True workforce stabilization requires looking beyond standard HR policies and addressing the physical and organizational design of the care environment. Conventional senior care facilities are often organized around institutional efficiency, characterized by centralized nursing stations, long, double-loaded corridors, and highly departmentalized, task-driven workflows. This structure fosters a culture of dependence for residents and turns clinical care into a series of repetitive, highly stressed tasks for staff.
Consider the transformation implemented at The Mount. They completely restructured their operational framework by implementing consistent caregiver assignments and cross-training staff to support residents across multiple care areas, putting the resident's preferences ahead of rigid departmental tasks. The clinical and financial outcomes of this shift were substantial:
- Clinical Quality Improvement: An internal evaluation comparing pre-implementation and post-implementation cohorts revealed that the number of residents requiring indwelling catheters fell from 12 to 1. Residents experiencing ADL decline dropped from 82 to 3, cases of significant weight loss fell from 20 to 3, residents requiring physical restraints fell from 22 to 2, and active pressure ulcers fell from 11 to 2.
- Workforce Stabilization: By shifting the staff's focus from rapid task execution to consistent, relational care, employee turnover plummeted from 50% to 15%. Under this model, the average tenure of a CNA at The Mount reached 7.6 years, far outperforming national averages.
- Financial Return on Investment: Reducing recruitment expenses, onboarding requirements, and agency reliance yielded an estimated operational savings of $270,000 per year.
Similarly, quantitative evaluations of the Green House Project (GHP) homes demonstrate their effectiveness in improving both clinical care and workforce retention:
- Pandemic-Era Workforce Stability: During the COVID-19 pandemic, when nursing homes experienced severe staffing crises, GHP homes reported turnover rates of 33.5% for Shahbazim (universal caregivers), 41.6% for LPNs, and 63.2% for RNs. This stands in sharp contrast to traditional nursing facilities, which suffered mean turnover rates of 129.1% for CNAs, 114.1% for LPNs, and 140.7% for RNs.
- Enhanced Direct Care Presence: Because the universal caregiver model integrates homemaking tasks and clinical support, GHP residents receive an average of 4.2 hours of direct care per day, compared to 2.2 hours in traditional facilities. This model adds 20 to 30 minutes of direct caregiver engagement per resident daily without increasing overall operating costs.
- Superior Clinical Outcomes: GHP residence is associated with a 5.5% decline in 30-day hospital readmissions, a 3.9% decline in avoidable hospitalizations, and a significant drop in the prevalence of bedfast residents, catheter usage, and pressure ulcers. During the pandemic, the GHP model's small-home footprint and stable staffing teams also contributed to lower infection and mortality rates compared to large institutional facilities.
Holistic Clinician Support: Onboarding Protocols and Mental Health Integration
Retention efforts are most critical during the initial phase of employment. Research shows that the first 100 days are the primary predictor of whether a new nurse or caregiver will remain with an organization, yet many senior care facilities overload new hires too quickly with heavy clinical assignments. Implementing structured onboarding programs can reduce early turnover by up to 25% compared to ad-hoc approaches.
An effective onboarding pathway requires a deliberate progression of responsibilities and structured support:
- 1. Pre-Start Engagement: Engagement must begin before day one. Organizations should send welcome materials, introduce the new hire to their immediate team via email, and confirm logistics such as parking, badge access, and first-day schedules to reduce anxiety and build early connection.
- 2. Clinical Shadowing Phase: New clinicians should not be assigned to solo care immediately. Experienced shadow-partners should accompany new hires for a minimum of two weeks, allowing them to learn documentation systems, clinical routines, and resident preferences.
- 3. Mentor Matching: Onboarding should pair new employees with seasoned mentors who serve as peer resources. Mentors provide guidance on clinical practices, organizational culture, and workflow management.
- 4. Calendarized Check-Ins: Administrators must schedule mandatory check-ins at 30, 60, and 90 days. These meetings should evaluate workload manageable levels, peer relationships, and clinical barriers.
In addition to clinical onboarding, addressing the psychological and emotional demands of senior care is essential for long-term retention. Frontline clinicians constantly navigate complex behavioral and emotional scenarios, particularly when caring for residents with dementia, substance use disorders, or serious mental illness. When staff feel unprepared to handle these challenges, they experience higher rates of stress and burnout. To support staff, facilities should integrate mental health training and wellness programs into their daily operations.
The Center of Excellence for Behavioral Health in Nursing Facilities (COE-NF)—established by SAMHSA and CMS—offers evidence-based training in de-escalation techniques, trauma-informed care, and substance use disorder management. Training staff in behavioral de-escalation helps reduce workplace violence, lowers staff burnout, and improves retention.
Simultaneously, administrators must establish supportive clinical systems that address staff wellness directly:
- Manageable Ratios and Workload Support: High workloads and staffing shortages create a cycle of physical and emotional exhaustion. Ensuring manageable caregiver-to-resident ratios prevents staff from being pushed past their breaking point.
- Structured Peer Support and Debriefings: Facilities should implement regular, non-punitive peer support sessions and team debriefings, allowing staff to process difficult clinical events, such as resident cognitive decline or end-of-life transitions.
- Accessible and Confidential Mental Health Resources: Leaders should connect employees to external, confidential counseling and support, such as programs that offer complimentary, non-reported mental health care for health professionals facing burnout.
- Culture of Feedback and Open Communication: Poor employer communication is a major driver of clinician distress and turnover. Establishing open-door policies, actively gathering feedback, and involving frontline staff in policy changes builds trust and improves organizational commitment.

Strategic Action Plan and Conclusions
To transition from a cycle of constant recruitment to a stable, retention-focused clinical environment, senior care executives should implement the following systemic recommendations:
- 1. Deploy Acuity-Adjusted Staffing Models: Eliminate rigid, average-based staffing schedules. Utilize dynamic translation frameworks to adjust nurse-to-resident ratios in real time based on resident care needs. Track workforce stability using a weighted, care-hour-based turnover metric to target retention efforts where care continuity is most at risk.
- 2. Establish Multi-Tiered Career Ladders: Partner with local workforce boards, community colleges, or state associations to implement structured CNA career pathways, such as the Kansas State CNA 1-4 model or California's competency-based upskilling program. Link clearly defined clinical milestones to automatic wage increases and expanded roles, such as restorative nursing, dementia care, or Qualified Medication Aide delegation.
- 3. Decentralize Care via the Small-Home Paradigm: Shift from traditional, institutional nursing unit designs to small, decentralized care environments. Implement consistent caregiver assignments, cross-train teams, and adopt the universal caregiver model to change daily work from a series of repetitive tasks to deep, relationship-based engagement.
- 4. Implement a Structured First-100-Day Onboarding Protocol: Standardize a comprehensive onboarding pathway for all new hires. This program should include pre-start communication, a minimum of two weeks of clinical shadowing, mentor matching, and mandatory 30, 60, and 90-day check-ins to address clinical concerns before they lead to resignation.
- 5. Integrate Frontline Behavioral Health and Wellness Systems: Train direct care staff in evidence-based de-escalation, trauma-informed care, and substance use management. Support these clinical skills with structured peer debriefings, manageable workloads, and confidential, non-reported mental health wellness resources to prevent moral injury and clinical burnout.
- 6. Leverage Workflow-Reducing Technologies: Deploy AI-enabled documentation, predictive analytics, and cloud-based communication tools to reduce the administrative burden on nursing staff. Use technology to simplify routine tasks, allowing clinicians to focus their energy on direct, high-value patient care. In my ten years in the Navy, we learned that operational readiness starts with preventative maintenance. You protect your assets before they break. Automating these front-end administrative tasks is how your teams reclaim the hours they need for mentorship and team culture.
- 7. Perform Local, Total-Rewards Benchmarking: Move beyond basic wage comparisons to design comprehensive, localized total rewards packages. Compare compensation, health benefits, PTO, and financial wellness tools against both local healthcare providers and non-healthcare competitors, replacing expensive signing bonuses with sustainable retention and referral incentives.
Operational Problem to Solution Matrix
Problem: High Early-Tenure Turnover
- Target Metric for Evaluation: 30, 60, 90-day retention rates.
- Systemic Solution / Action: Structured First-100-Day Onboarding, 2-week clinical shadowing, peer mentor pairing.
- Expected Clinical and Financial Outcome: Up to 25% reduction in early clinical turnover.
Problem: High Clinical Burnout & Injury
- Target Metric for Evaluation: Employee safety climate rating; injury rates.
- Systemic Solution / Action: Leadership safety commitment program, evidence-based SAMHSA de-escalation training.
- Expected Clinical and Financial Outcome: 10% overall reduction in nurse turnover; improved patient safety culture.
Problem: Flat Frontline Career Paths
- Target Metric for Evaluation: Number of CNAs promoted annually.
- Systemic Solution / Action: Multi-tiered career ladders; cross-training; state upskilling pathways (CNA 1 to 4).
- Expected Clinical and Financial Outcome: Improved direct care skills; long-term CNA retention; frees LPN/RN clinical time.
Problem: Agency Staffing Dependency
- Target Metric for Evaluation: Weighted annual turnover rate; contract labor hours.
- Systemic Solution / Action: Shift recruitment capital to internal salary, PTO, and total-rewards benchmarking.
- Expected Clinical and Financial Outcome: Reduced contract labor costs; improved team cohesion; higher Five-Star rating.
Problem: Institutional Rigidity
- Target Metric for Evaluation: Resident ADL scores; medication/hospital transfer rates.
- Systemic Solution / Action: Decentralize physical units into small neighborhoods; adopt the universal caregiver model.
- Expected Clinical and Financial Outcome: 50% to 15% drop in turnover; 31% fewer readmissions; $270,000 annual savings.